It shouldn't even be legal for health insurance providers to deny claims. It's essentially them practicing medicine without a license, because they're making calls about what healthcare a person needs or doesn't need, only a person's doctor(s) should be able to make those decisions.
Agreed. France, Germany, and Japan have health systems similar to the ACA, with the following differences: insurance is nonprofit with an effective mandate, there's a national price list for medical services, and claim denials are prohibited for anything on the list. Germany has an especially effective digital system that guarantees payment within a week.
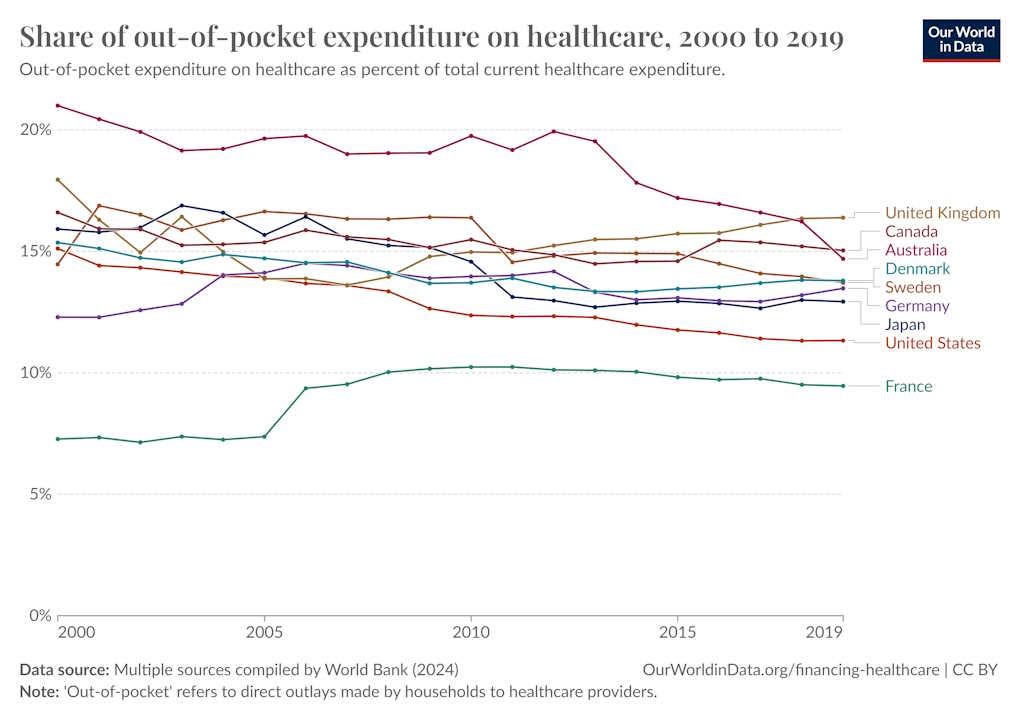
All three systems get better health results than the US, by measures like survival time after diagnosis of major disease. And all three spend a significantly lower percentage of their GDP on healthcare.
The other side of that is that some expensive services and drugs are simply unavailable in other countries, or are very tightly rationed. The USA has higher 5-year survival rates for most types of cancer than France, Germany, and Japan. I'm not saying that the US system is better overall, but it does do some things extremely well. We should make sure that any reforms don't sacrifice our unique advantages.
I'm not sure how implementing a system like Germany or Japan wouldn't impact those things at all. Why aren't Germany or Japan equal to the USA in 5-year cancer survival rates? Their systems optimize for different priorities, and those involve trade-offs.
So no, it obviously doesn't go without saying. If we want to cut overall health system costs or improve access then we might have to accept some reduction in service quality, at least for the most expensive stuff.
Perhaps because the US is the home of a number of prestigious colleges and to be with your peers you have to relocate there? You act like the broken healthcare system is the only possible explanation for cases where the US provides better care, but I'm yet to see that proven. Intuitively it doesn't track because many of the issues with the system don't pertain to things like intensive cancer care but to simple things that are of the exact same quality in countries with better systems, such as insulin where the only difference in the US is the price.
Not to mention, your comparison on cancer survival rates is flawed. The US system drives many people with cancer to be completely unable to afford treatment, which I doubt you've factored into your survival rate number.
Well now you're just making things up. It's not my cancer survival rate number, it's the number published by the CONCORD programme in the London School of Hygiene & Tropical Medicine. If you had bothered to read the article I linked above then you wouldn't need to doubt because you would know exactly what they factored in.
I did check it, it does not appear to mention this factor at all. I would assume then that they are focusing only on individuals who were able to actually get treatment, since this seems to be the survival rate among patients in treatment.
It seems to me that should then be handled by the legal system or perhaps the licensing boards. That is to say, the insurance companies should be forbidden from denying coverage and if they believe that something is going on then they can alert the police or take the doctor to court.
That's simply unrealistic. Medicine is more of an art than a science and most treatment plans fall into gray areas. While insurers do file formal complaints with authorities when there is clear evidence of fraud (like a single provider billing for more than 24 hours of patient encounters in a single day), there is an enormous amount of waste and abuse by providers which can't be proven in court as fraud. The fee-for-service financial model incentivizes over treatment.
The fundamental problem here is that demand for healthcare is virtually infinite while supply is limited. Healthcare already consumes about 20% of the US economy and there is no excess capacity to expand it further without dragging everything else down. We can make some things more efficient and reduce administrative burdens but ultimately we have to draw the line somewhere and ration care. That's going to be true regardless of whether we have commercial insurers or socialized healthcare.
Most doctors are not very rich at all, upper middle class. I make more than many doctors I know as a software engineer, and this doesn't even take into account their debt.
Care is expensive because of insurance. Hospitals needs hundreds of administrators and billing specialists. Very little of that money goes to the doctor.
Doctors deserve to be rich. They do incredibly specialized work where the outcomes are extremely critical, to put it mildly. I don't want doctors performing unnecessary treatments to line their pockets, but I don't think we're actually in danger of that.
The difference between a rich doctor and a rich insurance exec is that the doctor helps people, and the insurance exec makes their money withholding necessary care from people, in effect torturing and killing them.
This is the problem with insurance in general. The incentive of insurance is at direct odds with patients and doctors.
It's a tug of war, and even if insurance "loses", it doesn't matter, because you lost trillions of dollars in that tug of war. It's artificial inefficiency caused by privatization, very much a Dark Night burning a mountain of money situation.
Yes, insurance companies deny claims, but this is mostly because they don't have the money to pay for things most of their money is spent on care in the first place: they're forced to optimize and people get hurt in the process. Providers do far more damage.
UHCs profit margins are only 6%, their operating costs are extremely low[0], and if you look across G7 insurers in the US pay more than the government does in every country but France![1] Compare this to HCA which makes an average margin of 10% with far higher administrative costs. The CEO of HCA makes $20M, Brian Thompson made $10M by contrast.
This is not to say we (and insurance companies) don't spend astronomically more than other countries: providers are to blame for this, and I have seen their nonsense first hand:
- They keep people alive overnight to charge insurance more
- Some hospitals use ML (!) to optimize ICD codes for billing. Most do this by hand: there's literally a job and training to be an ICD coder.
- They allow people to deteriorate (e.g. dialysis) to charge more (no preventative care.) I have seen a hospital only provide preemptive care to patients at risk of dialysis because they were part of their own insurance pool
- Their administraive expenses are far higher.
- They test and provide unnecessary care.
- Physician shortage is in part caused by limited residency spots, a dumb bachelors requirement, and high tuition costs. These barriers to entry are imposed by physicians.
- Uneccesary tech and equipment upgrades (e.g. we need to replace your knee with a new knee)
- Having to deal with tons of different insurance companies: not their fault but they don't know how to handle this efficiently.
Because customer-insurer relationships are the only side of the healthcare system that most people see, they're oblivious to what are actually pass-through insurer-provider issues.
As you said, the reality is that insurers operate with pretty reasonable margins and incredibly meager per-claim overhead costs. They're stuck trying to make 2 + 1 = 2.
If the finger should be pointed at root causes in the US health system, it should be at:
- Providers overbilling (particular in certain specialties)
- Medical schools, for charging too much and under-expanding capacity
- The federal government/Congress, for failing to expand residency funding to increase supply (especially in generalist provider categories)
What’s the source of limited supply of doctors meme? Is there a good rundown somewhere?
Because anecdotally, among my friends, I’ve never known someone to not make it through the system to practicing medicine who wanted to, but I do know several who persevered despite being real idiots. I don’t see how opening the pool wider would lead to better care.
1. There is a cap on the number of doctors that the US can churn out since Medicare funds most of their training. That number is 140,000. This inherently limits supply. This is the biggest issue.[0]
2. There are limited spots in certain residency programs due to how competitive they are. Ergo those specialties are artificially more lucrative. Dermatology is a good example.
3. Becoming a doctor is temporally arduous: 11 to 15 years! Why the hell do people need to spend four years of time and money on a bachelor's degree instead of entering a medical program directly?
4. Becoming a doctor is financially arduous. You will be in debt for four years of undergrad, then four years of medical school, and then you'll be paid garbage for 3-7 years of residency. High interest rates exacerbate this.
5. Residency is hell.
6. Working in a hospital is often hell. Burn out is very real.
7. There are many, many professions which provide a far better standard of living.
Agreed. There are a few schools now offering accelerated Baccalaureate-MD programs in as little as 6 years so expanding those to more schools would be a relatively simple way to cut education costs.
We can also expand access to affordable primary care by shifting routine services to physician assistants and nurse practitioners. Physicians should be reserved for more complex or higher risk cases.
1. This is true sometimes, but still privatization and insurance's fault. Hospitals have a motive to charge insurance more money. Public healthcare doesn't have this problem.
2. Administration and billing is ludicrously expensive because of insurance. Thousands of insurers with their own processes breeds the most inefficient and broken system you could possibly imagine. The solution is removing the market, i.e. having a single payer. Boom, administration costs disappear.
3. Preventative care is rarely paid for by insurance. In addition, many patients simply don't do it. It's easy for a smoker to get treatment for COPD, it hard for a smoker to stop smoking. That's just how it is.
No matter how you slice the healthcare problem in America, it undebatable that private insurance must go. The inefficiency it creates is absurd and it's why our healthcare costs are through the roof.
Not only do we pay much, much, MUCH more per citizen for care, but our care is also lower quality as compared to the rest of the west.
Expanding, essentially the US has the worst of all possible worlds.
Most provider costs are obscured / complicated by insurers sitting in the middle of transactions.
If they weren't, providers wouldn't do some of the all-but fraudulent coding shenanigans that have become normalized. But overbilling a faceless insurer is fine.
And likewise, patients would have an incentive to shop around for the most cost effective services, instead of no one in the system being able to proactively say how much something would cost until the insurance claim is submitted and processed.
USA Anti-trust is on life support and there is generally very little political willpower to disentrench incumbent capital interests.
Wealthy lobbyists for providers and health insurance companies prevent any change basically.
Also misguided American exceptionalism whereas people think the healthcare standards will go down significantly if there is a public option (as if they weren't already down for the things people can actually afford).
Sounds like the business model they’ve decided to use might not be viable.
I mean, actually it makes sense. Their job is to pay for expensive procedures, sometimes quite urgently needed. They can’t really ethically insert themselves into the decision making process, so if these companies were run ethically they’d be signing themselves up for unlimited risk.
Please allow me to counter, from the perspective of someone who owned a medical practice for much of my adult life:
- The ACA limits the amount of money, as a percent of revenue, that insurance companies collect as profit. If they wish to increase profit, their primary option is to collect higher premiums and pay more benefits.
- (No experience with keeping someone alive overnight. I'm sure it's happened and couldn't disprove it in any case.)
- Of course they have optimized billing. The current fiasco has byzantine rules for payment. For instance, you know how your dermatologist offers you smoking cessation and weight loss classes? That's because if they offer it to you, insurance rules allow them to bill the encounter as an enhanced care visit which pays more. This isn't an exaggeration. The insurance rules say "we'll pay you an extra 30% if you ask about their smoking and weight". The doctor can earn more simply by following those rules. Again, of course providers do this! If my boss gave me a 20% raise for asking him each morning if he'd like me to make him a sandwich, even knowing he hates breakfast sandwiches, you bet I'm doing it.
- That's complicated. If a hospital violates the insurer's rules, they don't get paid for seeing the patient. Yes, the situation you described is horrid, but no provider can afford to write off every patient. It's the insurers who said they wouldn't pay until the patient is seriously sick.
- Surveys have shown that as much as 60% of small practices' management overhead involves staffing people to deal with insurance companies, process claims, optimize billing (see above), negotiate pre-approvals, and so on. They have higher overheads because the insurers require it, not because they want to.
- Well, according to the insurers trying to weasel out of paying for it. For example, a patient came to my wife with an obvious soft tissue injury. She ordered an MRI to diagnose it. The insurer refused the approval until my wife took an X-ray first because it's cheaper. X-rays also don't show soft tissue injuries. (Don't correct me; I know the exceptions here and they're not relevant to this.) So it was the insurer who demanded my wife perform a wholly useless test before they'd pay for the effective one.
- I'm not willing to lower the quality of physicians. Other studies have shown that the lack of upcoming doctors is due to fewer people willing to put up with the insane stress levels for mediocre pay. The stereotype of a doctor heading out at noon for an afternoon of golf are largely over for nearly all specialties. Frankly, there are many jobs that pay better with less stress and less personal responsibility.
- That's laughably wrong. No one gets a new knee for the fun of it. It's a major surgery with long and challenging recovery that people get because they're otherwise unable to function normally.
- There is no way to handle this efficiently. It's an utter morass.
- I'm not willing to lower the quality of physicians. Other studies have shown that the lack of upcoming doctors is due to fewer people willing to put up with the insane stress levels for mediocre pay. The stereotype of a doctor heading out at noon for an afternoon of golf are largely over for nearly all specialties. Frankly, there are many jobs that pay better with less stress and less personal responsibility.
This assumes that the things being done now are meaningfully contributing to the quality of physicians vs various proposals.
It's also probably a mistake to measure the quality of the doctor vs the quality of the care that is delivered. More doctors that are less stressed and can spend more time on each patient could easily outperform a smaller group of "better" doctors.
> Otoh some medical providers like to over bill and over treat.
This is true to some extent, but the share of medical providers that over-bill and over-treat really doesn't justify the way the insurance industry does business. It's a false equivalence.
Yes, but in my opinion it falls to the patient to figure out the details and absorb the risk. That's the messed up part. That insurance providers and medical services might disagree on pricing or whatnot is an inevitability. What's not fair is throwing ordinary people under the bus to deal with it, which for many reasons is risky and can ruin lives.
Stop speciously muddying the waters by either intentionally or accidentally making spurious arguments for these unethical sociopaths.
I’ve seen this argument made on this website a lot, and it always conveniently omits the vertical integration of these insurers wherein they are the providers too.
The DOJ is literally, actively, suing to block a merger between united healthcare and a provider.
It's not clear that vertical integration is necessarily bad for consumers. For example, Kaiser-Permanente is a huge, vertically-integrated "payvider" which both sells insurance plans and also delivers most of the treatment for plan members. They generally do a pretty good job at a competitive price.
Both the payer and provider sides of the healthcare industry have been consolidating for years. Insurers merged to gain more negotiating power with providers and drive down costs. Providers responded by merging (or selling to private equity funds) to gain more negotiating power with insurers and maintain high rates. Government mandates on back office technology also incentivized provider consolidation due to economies of scale. In some areas now a few major provider organizations effectively control the market and payers are essentially forced to pay high rates in order to maintain sufficient networks. So, the logical next step is for payers to mimic KP by building their own captive health systems. Every major payer is pursuing this strategy to varying levels; it's not just UHC.
I'm glad to see this phrased this way, because that was something I felt but hadn't articulated consciously. It's literally private accountants making healthcare decisions.
All large health insurers employ many physicians. You're not wrong that they may not have all of the evidence but there is a lot of licensed medical knowledge available to all Payors.
That’s the crux of it. I didn’t visit with any of my insurer’s staff, like I did with my own doctor. How are they making treatment decisions without ever having seen the patient?
{kind=link}